Neurology brings together the art of human interaction and expression on one hand with the clinical assessment, advanced neuroimaging, understanding of disease and therapeutics on the other hand. Here are some notes focused on the study of nervous system disease, the natural history and pathological mechanisms; our Neuropathology notes!
Neuropathology notes:
Stains:
- H&E hematoxylin & eosin stain:
- Basophilic: stains blue/purple, takes up the base (hematoxylin)
- Eosinophilic: stains pink/red, takes up the acid (eosin)
Biopsies:
An approach to Brain biopsies:
PAS-positive macrophages in the brain are found in:
- Whipple’s disease
- Adrenoleukodystrophy, Globoid-cell leukodystrophy, metachromatic leukodystrophy, and other hereditary leukodystrophies
- Acquired leukoencephalopathy due to toxins e.g. organic solvents
Ballooned neurons are found in:
- Argyrophilic grain disease AGD
- Progressive supranuclear palsy PSP
- Corticobasal degeneration CBD
- Parkinson’s disease
Coiled bodies in oligodendrocytes are found in:
- Tauopathies
- Argyrophilic grain disease AGD
Lymphocytic markers:
- Pan B-cell antigens (CD19, CD20, CD22, CD79a),
- CLA leukocyte common antigen or LCA= CD45
- In Diffuse large cell B cell lymphoma:
- CD5+ leads= worse prognosis
An approach to Muscle biopsies :
General notes on muscle biopsies:
Suitable biopsies:
- Don’t biopsy a site of previous EMG needle insertion (focal necrosis & inflammation occur)
- Don’t biopsy severely affected end stage muscle
- Don’t biopsy uninvolved muscle
- Don’t biopsy near tendinous insertions (fibre size variation)
- Don’t biopsy gastrocneimus
- i.e. biopsy MRC 3 grade muscle
- Size of biopsy: 1cm X 1cm X 1-2.5cm is sufficient. Don’t manipulate or traumatize the muscle too much.
Staining of frozen sections with 8 stains:
- 5 stains.
- 3 muscle enzyme histochemical reactions
This can be followed by:
- More histochemistry
- Immunohistochemistry IHC
- Electron microscopy EM
- Molecular tests: Western blott, Southern blott, PCR,
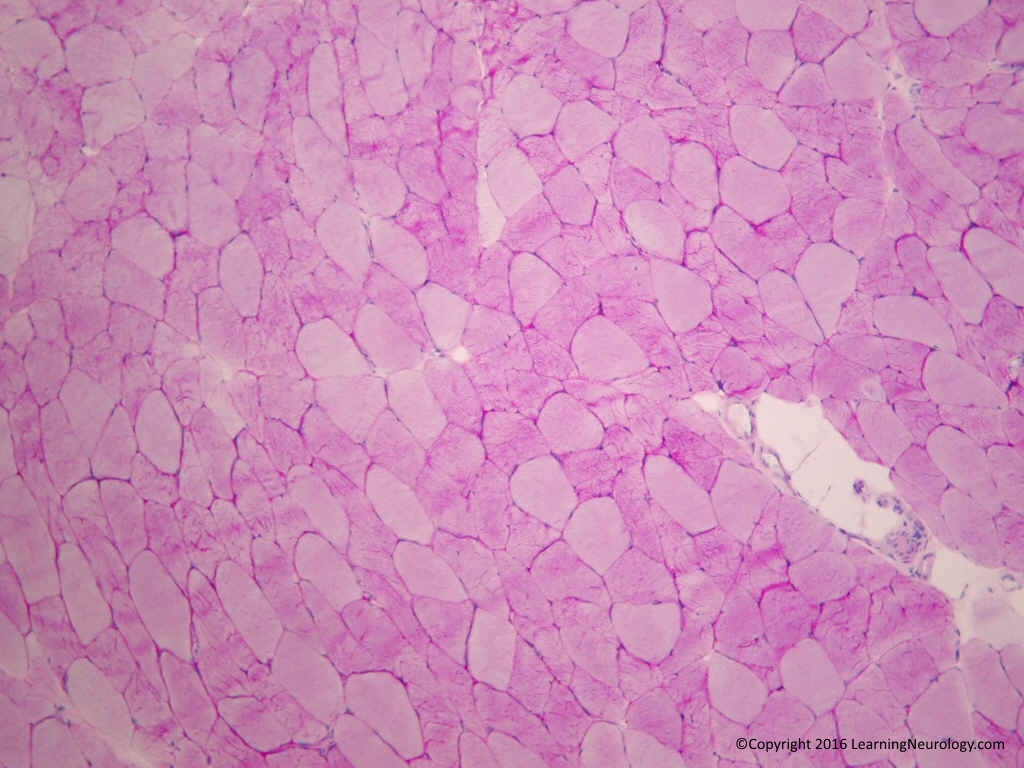
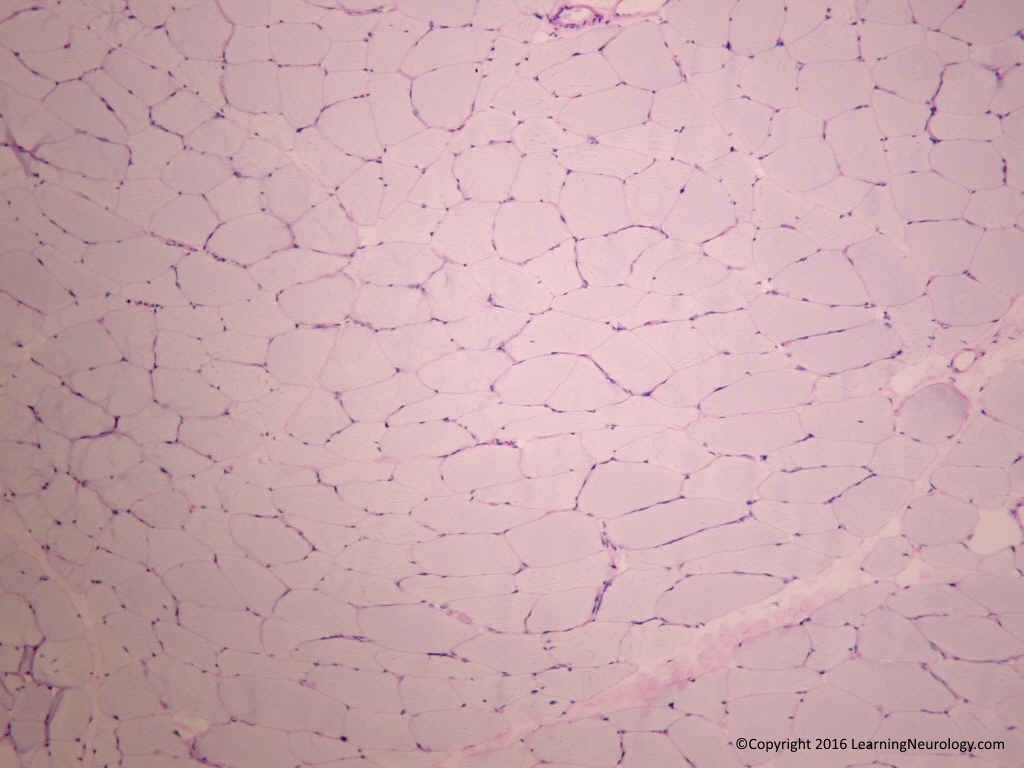
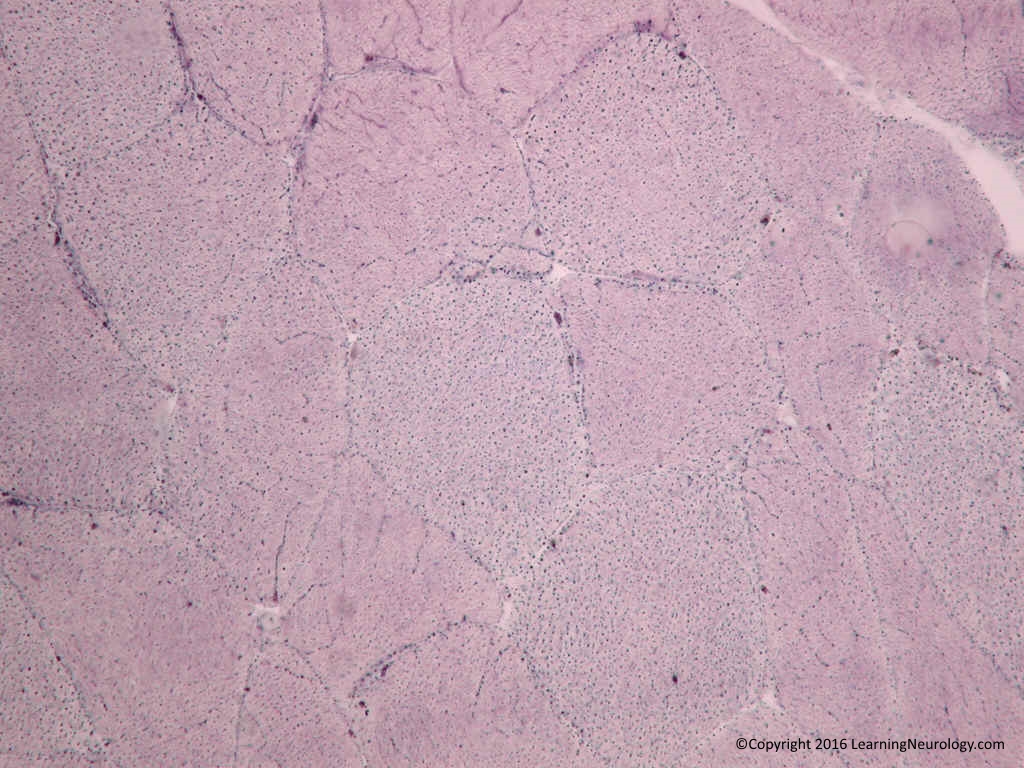
Hematoxylin & Eosin (H&E) stain :
Muscle fibres size:
- Variation is size (diameter).
Muscle fibre shape:
- Polygonal in adults
- Round:
- Normal: in infants & very young children
- Round: in myopathies e.g. muscular dystrophies
- Angulated: small angulated in neuropathy
Muscle fibre structure:
Atrophic fibres:
- “nuclear bags” without much myofibril
Note distribution of atrophy:
- Random
- Fascicular ‘group atrophy’: denervation
- Perifascicular atrophy (perimysium): dermatomyositis
Note type of fibre atrophy (see other stains)
Regenerating fibres:
- Basophilic (blue) fibres
- These occur in myopathies
Necrotic fibres:
- Eosinophilic homogenous cytoplasm, in longitudinal section (loss of striations). Later: vacuolated fibres, infiltration with inflammatory cells (macrophages & lymphocytes).
- Dystrophic, Inflammatory or toxic myopathy.
Split fibres:
- These occur in muscular dystrophies
Rimmed vacuoles:
- Vacuoles rimmed by basophilic material. Inclusion body myositis,
Vacuoles without rims:
- Metabolic myopathies:
- Glycogen storage diseases,
- Hypokalemia
- Drugs (lysosomal toxicity): colchicine, chloroquine, amiodarone
- Hyperkalemia periodic paralysis/hypokalemic periodic paralysis
Centromyocytic necrosis:
- Inflammatory cells in the myofibre surrounded by normal sarcoplasm occurs in polymyositis.
Ragged red fibres:
- best seen on Gomori’s trichrome stain. Subsarcolemmal +/-intermyofibrillary aggregates, blue on H&E. Occurs in Mitochondrial disorders & in patients >60 y.o..
Whorled fibres ‘coiled fibres’: central disorganisation of myofilaments.
Location of nuclei:
- Peripheral: normal
- Central: muscular dystrophies, myotinic dystrophy
Connective tissue on H&E:
- Endomysium: increased connective tissue ‘endomysial fibrosis’ occurs in muscular dystrophies.
- Perifascicular (perimysium):
- Look for inflammation around vessels in inflammmatory myopathies.
- Look for inflammation involving vessels in vasculitis, destruction of vessel wall, fibrinoid necrosis.
- Epimysium (fascia)
Gomori’s trichrome stain:

Stains mitochondria red.
- Rimmed vacuoles: vacuole rimmed by red staining material. Inclusion body myositis,
- Ragged red fibres: Subsarcolemmal +/-intermyofibrillary aggregates, appear red. Occurs in Mitochondrial disorders & in patients >60 y.o..
- Target fibres: central lack of staining, surrounded by dark intermediate zone, surrounded by normal staining peripherally. Denervation.
- Nemaline rods: sarcoplasmic red aggregations
PAS stain:
Stains glycogen & mucin. Stains type II fibres well.
- Increase staining: glycogen storage diseases
- No staining: necrotic fibres
PAS D stain:
Stains mucin but not glycogen i.e. if something is dark on PAS and on PAS D, it is mucin.
Oil Red O stain:
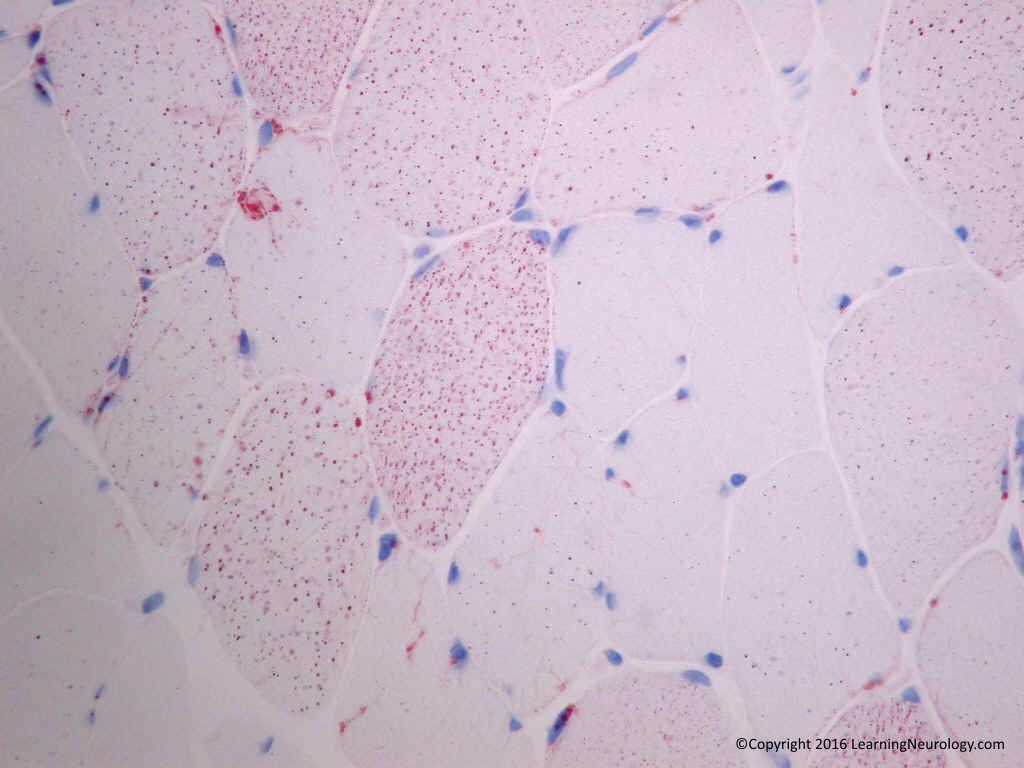
Stains lipid well.
- Increased staining:
- Lipid storage diseases
- Mitochondrial diseases
NADH-TR stain (NADH tetrazolium reductase):
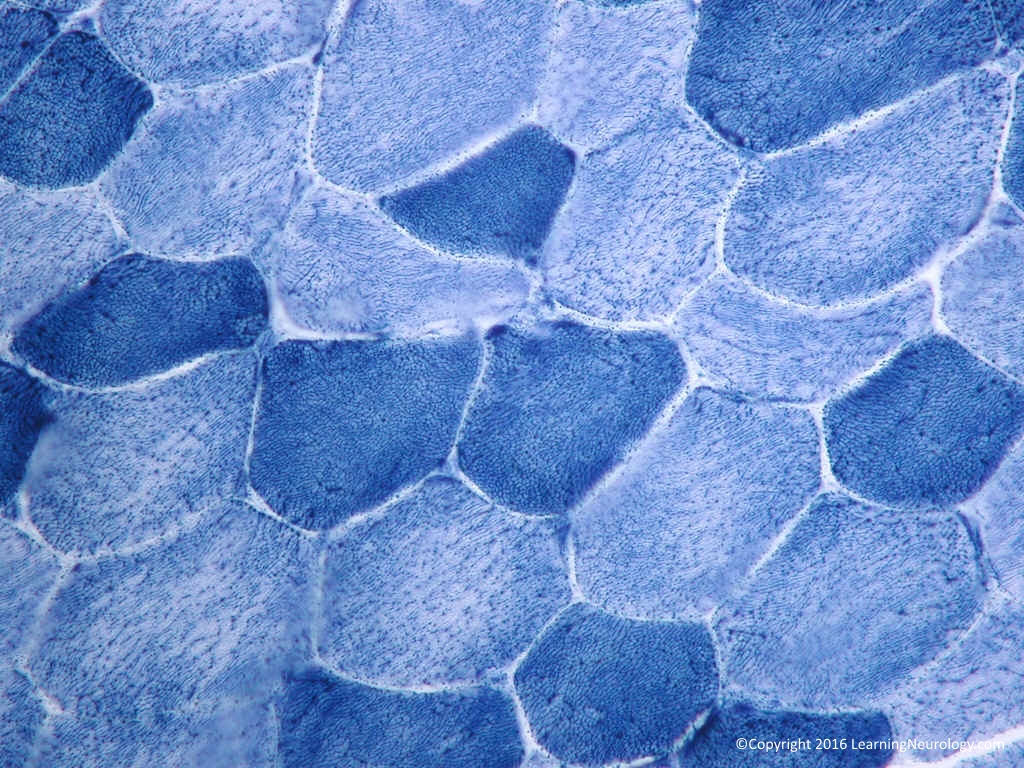
Stains type I fibres well. Good for structure:
- Target fibres:
- Central lack of staining, surrounded by dark intermediate zone, surrounded by normal staining peripherally.
- Central cores:
- Lack of staining in the centre.
- Occurs in Central core disease
- Central clearing:
- Occurs in Denevation
- Ring fibres:
- Subsarcolemmal peripheral rim of increased staining, myofibrils perpendicular to the axis
- Occurs in Myotonic dystrophy
- Necrotic fibres:
- No staining.
- Occurs in dystrophic, inflammatory or toxic myopathy
- Moth eaten fibres:
- Ill defined areas of loss of staining.
- Non-specific: Inflammatory myopathies, malignant hyperpyrexia, denervation
- Lobulated fibres:
- Irregularities of the intermyofibrillary network
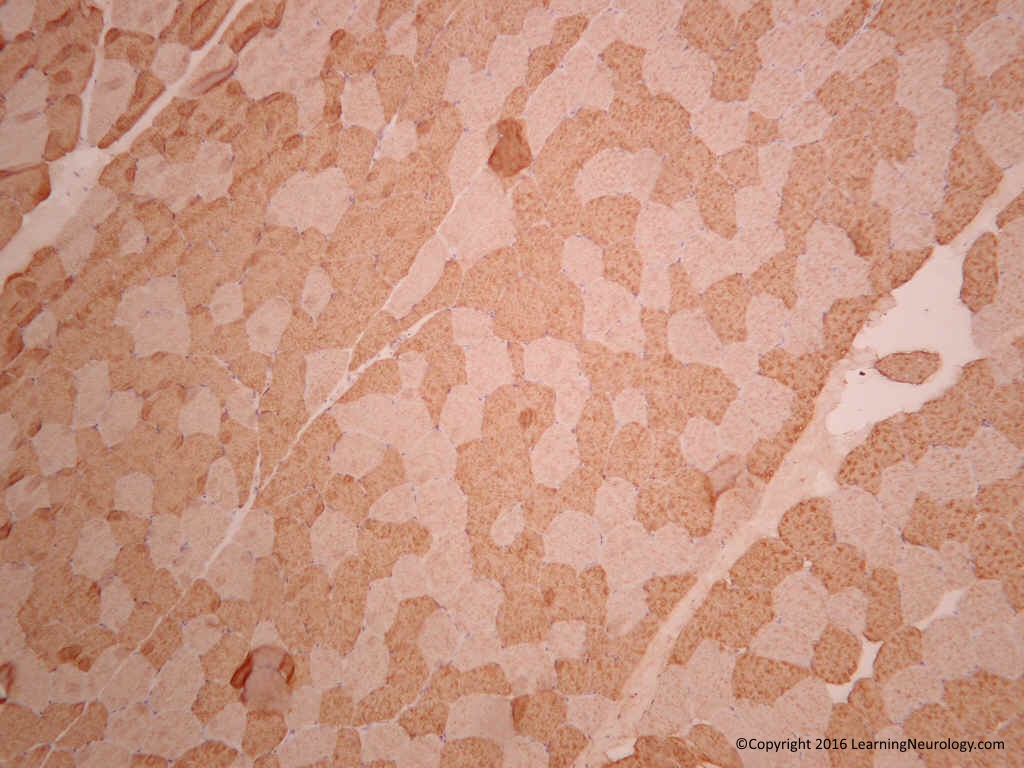
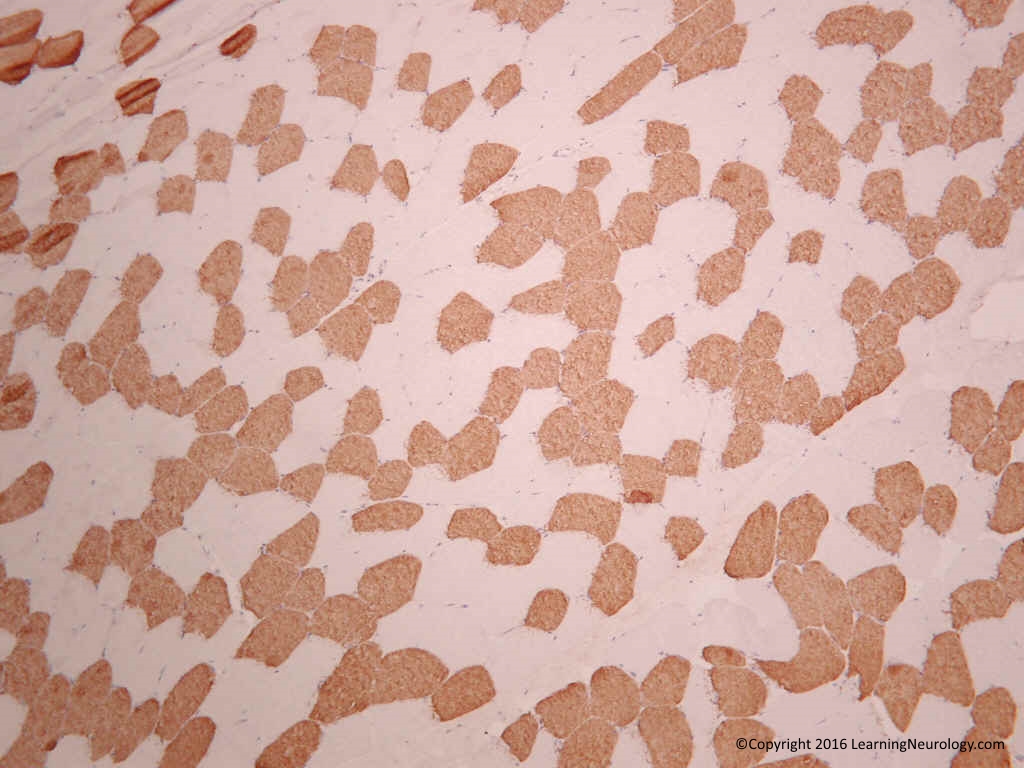
ATPase stain:
- Fibre type grouping: denervation & renervation
Type I fibre atrophy:
- Myotonic dystrophy
- Congenital myopathies
- Deneravation
Type II fibre atrophy (usually type IIb):
- Non-specific
- Occurs in Disuse atrophy
- Occurs in steroid induced myopathy
- Lots of other stuff
Type I fibre predominance:
- i.e. more type I than usual:
- Occurs in Congenital myopathies
Type II fibre predominance:
- i.e. more type II than usual:
- Occurs in Amyotrophic lateral sclerosis
Notes:
- Axonal neuropathies cause fibre type grouping. In demyelinating neuropathies fibre type gourping doesn’t occur because the axons and hense the neurotropic factors are intact.
COX SDH stain (cytochrome c oxidase, succinate dehydrogenase):

COX stains brown, SDH stains black. COX stains mitochondria.
- COX deficient fibres
- Moth eaten fibres
| Fibre type | Type I (slow twitch) | Type II (fast twitch) |
| Mitochondria | High | Low |
| ATPase at 4.3 | Dark | Light, except type IIc fibres |
| ATPase 10.3 | Light | Dark |
| ATPase 4.6 | Dark | Type IIa are light Type IIb are intermediately staining |
| COX SDH | Dark | Light, unless atrophic |
| Fast myosin | None | High |
| Glycogen | Rich |
| Myopathic pattern | Neuropathic pattern |
| Extensive variation in fibre size | Nests of atrophic fibres |
| Rounded fibres | Angular fibres |
| Central nuclei | No central nuclei |
| Necrotic fibres | No necrotic fibres |
| Cytoplasmic alteration | Target cells |
| Interstitial fibrosis | Minimal interstitial fibrosis |
| Inflammatory cell infiltrates | No inflammatory cells |
Muscle immunohistochemistry:
Fast myosin:
- Present in type II (fast twitch fibres)
Slow myosin:
- Present in type I (slow twitch fibres)
NCAM isoform CD56/Leu19:
- Marker of satellite cells (beneath basal lamina), indicating regeneration of muscle
Muscle histochemistry:
Myoadenylate deaminase MAD:
Phosphofructokinase PFK:
Myophosphorylase MPH:
An approach to Nerve biopsies:
Patterns of nerve damage:
Neurapraxia:
- Damage to myelin only, causes conduction block
Axonotmesis:
- Damage to axons with intact myelin & connective tissue. Wallerian degeneration occurs distal to the lesion.
Neurotmesis:
- Damage to axon, myelin & connective tissue i.e. complete nerve damage.
Others:
- Uniform demyelination (all nerves, e.g. Charcot-Marie-Tooth)
- Segmental demyelination (some fibres affected others not)
- Focal demyelination (all fibres in one focal area are affected)
- Conduction block (severe form of focal demyelination)
General notes on nerve biopsies:
- Sizes of nerves:
- Myelinated fibres 2-15 microns:
- Large & small, usually 1:2 ratio
- Unmyelinated fibres 0.5-2 microns, more abundant than myelinated fibres
- Myelinated fibres 2-15 microns:
- Nerves by myelination:
- Myelinated:
- Motor nerves are myelinated
- Myelinated:
Vibration & proprioception nerves are myelinated
- Unmyelinated:
- Pain & temperature nerves are unmyelinated
Autonomic nerves are unmyelinated
- Structure:
- Epinurium
Perinurium
Endonerium
- Stains:
- Paraffin fixed nerve:
- H&E (frozen or permanent sections)
- Permanent sections are good for inflammatory cell infiltrate, granuloma, lymphoma
- H&E (frozen or permanent sections)
- Paraffin fixed nerve:
Vasculitis: transmural inflammation of the vessel wall & fibrinoid necrosis,
- LFB luxol fast blue:
- for myelin (blue)
- Trichrome stain:
- Bodian stain (a type of Silver stain):
- for axons
- Congo-red stain:
- Amyloidosis
- Alcian blue, Cresyl violet, PAS
Immunohistochemistry:
- Neurofilament immunohistochemistry: for axons (large & small)
- S100 protein: Schwann cells & Schwannomas
- CD20: B cells
- CD3: T cells
- EMA: perineural cells & perineuromas
- Osmium: ?what is it embedded in
- for myelin
- Gluteraldehyde:
- Semithin (10 micro M) plastic preparations:
- for myelin & demeylinating neuropathies
- Semithin (10 micro M) plastic preparations:
Assess population of myelinated fibres i.e. small vs. large myelinated fibres (& myelinated fibre loss)
Demyelination:
- Denuded axons (Normal nonmyelinated axons are 0.5-2 microns in diameter. If a fibre >3 micron is found without myelin then it is a denuded axon)
- Thinly myelin axons i.e. remyelinating i.e. there was previous demyelination
- Giant axons
- Tomacula
- Polyglucosan bodies
- Onion bulb formation
- Axonal sprouting= clusters of Small thinly myelinated axonal sprouts (evidence of chronic axonal degeneration)
- Myelin ovoids may be confused with crush artefact
- G ratio= Axon to entire nerve fibre ration = 0.6
- G Ratio >0.6 implies thinly myelinated axon
- G Ratio <0.6 implies axonal damage
- On frozen nerve:
- H&E
Modified Gomori Trichrome stain:
- For myelin (pink/red)
- Myelin-digestion chambers
- Tomacula
- Giant axons
- Polyglucosan bodies
- Onion bulb formations (red-tinged myelin surrounded by Schwann cell nuclei)
Central fascicular degeneration, & selective nerve fascicular degeneration: ischemia
- Cresyl-fast violet:
- Shows metachromatic substance
- PAS:
- Polyglucosan bodies
- Congo-red stain:
- Amyloidosis
- EM electron microscopy:
- Thin (1 micro M)
G ratio= Axon to entire nerve fibre ration = 0.6
G Ratio >0.6 implies thinly myelinated axon
G Ratio <0.6 implies axonal damage
Small thinly myelinated axonal sprouts (chronic axonal disease)
- Teasing technique a.k.a. Teased preparation:
- =or>100 fibres need to be evaluated
Shows mild demyelination & axonal degeneration
Demyelination:
- Decreased internode distance (remyelination)
- Wallerian degeneration: myelin ovoids are seen
Tomacula (excessive folds of myelin) can be seen (HNPP)
Interpretation:
- Hemosiderin in nerve: old evidence of vasculitis
- Patchy loss of axons: vasculititis
Skin biopsy for neuropathy:
- 3mm punch skin biopsy from leg skin
- Anti-protein-gene-product 9.5 protein a.k.a. Anti PGP 9.5 by immunohistochemistry or immunofluorescence, (this stains nerve fibres in the skin)
- Count intraepineural nerve fibres IENF
- Reduced: <8 fibres/mm on dorsum of foot
- If reduced small fibre sensory neuropathy is present (with or without other features of distal symmetric polyneuropathy). If not reduced, distal symmetric neuropathy is still possible.
CNS immunohistochemistry:
| Antibody/antigen | Tumours positive | Tumours negative |
| GFAP | Astrocytoma, oligodendroglioma, glioblastoma | Meningioma |
| Synaptophysin | ||
| Neurofilament | ||
| Chromogranin | Paraganglioma | |
| EMA | Meningioma* | Solitary fibrous tumor |
| Vimentin | Meningioma, hemangiopericytoma, solitary fibrous tumor | |
| Cytokeratin | ||
| S100 | Schwannoma | Solitary fibrous tumor |
| CD99 | ||
| Smooth muscle specific actin | ||
| Desmin | ||
| Myoglobin | ||
| INI1 | Atypical teratoid rhabdoid tumor ATRT* | |
| CD1a | Langerhan cell*, | |
| AE1/AE3 | ||
| CD34 | Solitary fibrous tumor* | Hemangiopericytoma (only mildly), |
| Ki-67 (MIB index) | Tumors with frequent mitosis |
* important association
Lymphocyte markers:
Pan B-cell antigens (CD19, CD20, CD22, CD79a),
CLA leukocyte common antigen or LCA= CD45
In Diffuse large cell B cell lymphoma:
CD5+ leads= worse prognosis
Neuroimmunology:
Multiple sclerosis:
- Plaques within white matter: demyelination, lymphocytes (T & B Cells), activated macrophages/microglia,
- Oligodendrocyte loss
- Axonal loss, gliosis, astrocyte proliferation
Paraneoplastic syndromes & antibodies:
| Syndrome | Antibodies (synonym) |
| Paraneoplastic encephalomyelitis | Anti-Hu Anti-amphiphysin Anti-CRMP5 (anti-CV2) Anti-PCA-2 ANNA-3 Anti-NMDAR |
| Paraneoplastic Cerebellar degeneration | Anti-Hu Anti-Yo (PCA-1) Anti-Tr Anti-CRMP5 (anti-CV2) Anti-PCA-2 Anti-Ma1 Anti-mGluR1 |
| Paraneoplastic sensory neuropathy | Anti-Hu Anti-CRMP5 (anti-CV2) ANNA-3 |
| Paraneoplastic autonomic neuropathy | Anti-Hu Anti-nicotinic ACh receptor Purkinje cell antibodies PCA-2 |
| Paraneoplastic intestinal pseudoobstruction | Anti-Hu |
| Lambert-Eaton Myasthenic syndrome LEMS | Anti-VGCC Anti-PCA-2 |
| Myasthenia Gravis | Anti-ACh receptor Anti-titin |
| Antibodies (synonym) | Paraneoplastic syndrome | Underlying cancer |
| Anti-Hu* (ANNA-1) | Sensory neuronopathy Autonomic dysfunction Encephalomyelitis Cerebellar degeneration Myelitis |
Small cell lung cancer Neuroblastoma Prostate cancer |
| Anti-Yo (PCA-1) | Cerebellar degeneration | |
| Anti-PCA-2 | Encephalomyelitis Cerebellar degeneration LEMS |
Small cell lung cancer |
| Anti-amphiphysin | Stiff-man syndrome Encephalomyelitis |
Breast cancer Small cell lung caner |
| Anti-gangliosides | Sensorimotor neuropathy | |
| Anti-VGKC | Neuromyotonia | Thymoma Small cell lung caner |
| Anti-VGCC | Lambert Eaton Myesthesenic Syndrome LEMS | Small cell lung cancer |
| Anti-ACh receptor | Myasthenia gravis | |
| Anti-titin | Myasthenia gravis | |
| Anti-neuronal nicotinic Ach receptor | Autonomic dysfunction and several other disorders | |
| Anti-MAG | Sensorimotor neuropathy | Waldenstroms macroglobulinemia |
| Anti-Ri | Ataxia Opsoclonus-myoclonus |
Breast Gynaecologic Lung cancer Bladder cancer |
| Anti-Tr | Cerebellar degeneration | Hodgkin’s lymphoma |
| Anti-retinal a.k.a. Anti-CAR (anti-recoverin protein) | Cancer-associated retinopathy Melanoma-associated retinopathy |
Small cell lung caner Melanoma Gynecological |
| Anti-CRMP5 (anti-CV2) | Encephalomyelitis Cerebellar degeneration Chorea Sensory neuropathy |
Small cell lung cancer Thymoma |
| Anti-Ma1 | Brain stem encephalitis Cerebellar degeneration |
Lung cancer Other cancer |
| Anti-Ma2 (a.k.a. anti-Ta) | Limbic brain stem encephalitis | Testicular cancer |
| ANNA-3 | Sensory neuronopathy Encephalomyelitis |
Lung cancer |
| Anti-mGluR1 | Cerebellar degeneration | Hodgkin’s lymphoma |
| Anti-NMDAR | Limbic encephalitis (Associated with orolingual dyskinesias & catatonia like state) | Ovarian teratoma |
Other notes:
- VGKC, voltage-gated potassium channels (Kv1) antibodies: These are positive in patients with limbic encephalitis, Morovan’s syndrome. These have differnet targets.
- Caspr2: contactin-associated protein-antibody-2, a subtype of VGKC found in Morovan’s syndrome
Lgi1: leucine-rich, glioma inactivated 1 protein, a subtype of VGKC found in limbic encephalitis.