To correctly interpret CT of the head a systematic approach is most useful. In this section we outline an approach used by many neuroradiologists and neurologists to interpret CT head. Of course, you’ll have to hit the books, review articles and original research and interpret hundreds of scans to get the real expertise, but here’s a start!
Introductory notes:
- Bright areas are called: hyperdense, high density, or high attenuation
- Dark areas are called: hypodense, low density, or low attenuation.
- Window: this is a term use to describe the settings when viewing the CT scan. You can set up the window for “a lung window”. This will show up the features of the lung really well, but the features of the mediastinum poorly & vice versa.
CT interpretation steps:
Description:
- Patient details
- Date of CT
- Technical features, Type: contrast vs. non-contrast
- Imaging features:
- Go through all the structures
- Describe lesions that are found
Approach to the structures:
Approach the following areas systematically:
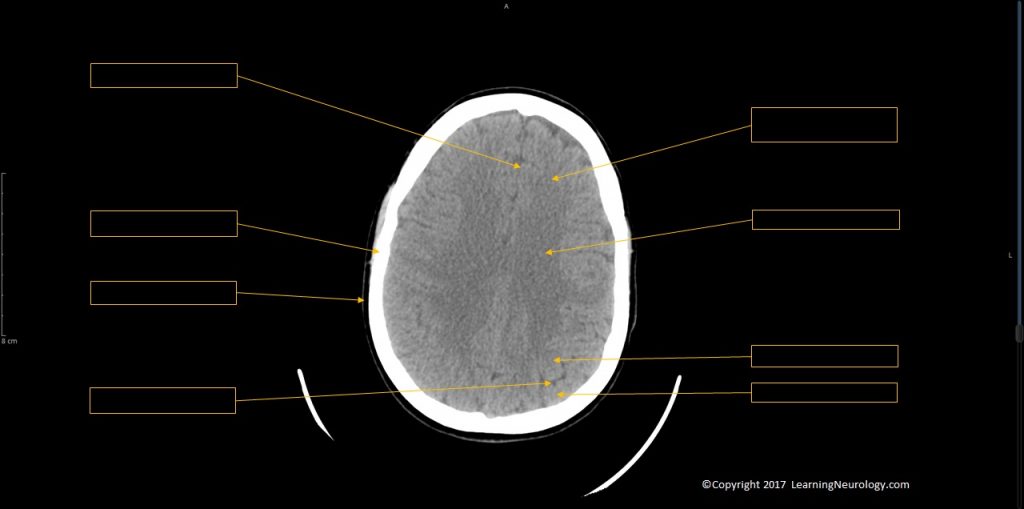
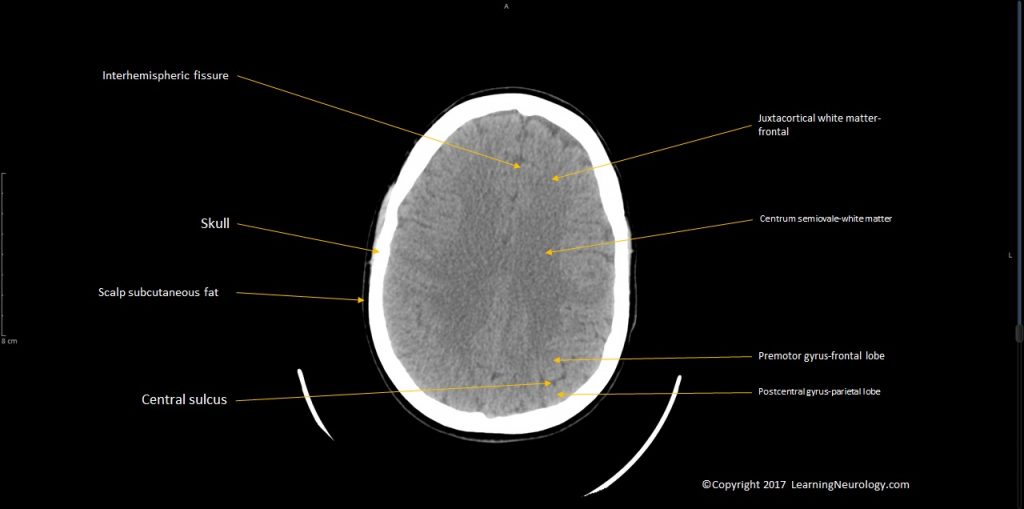
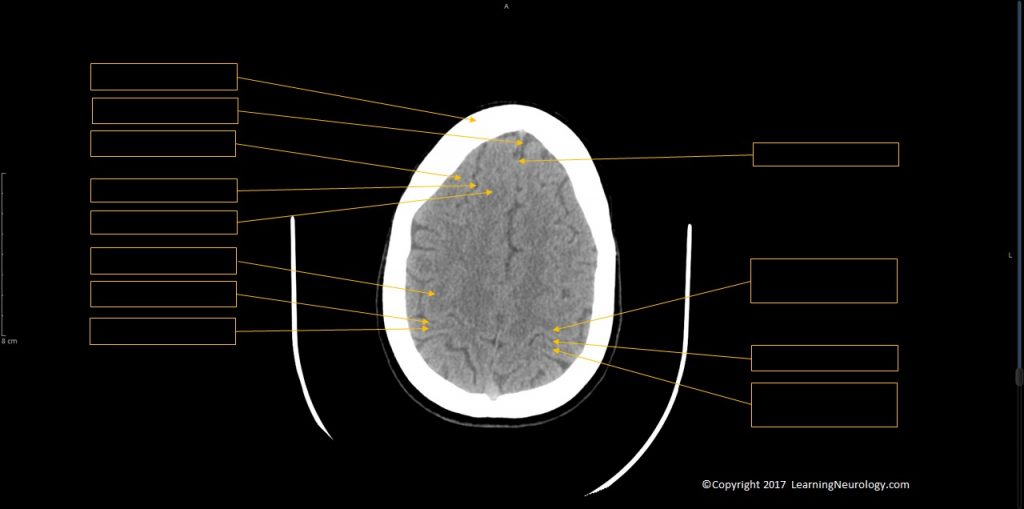
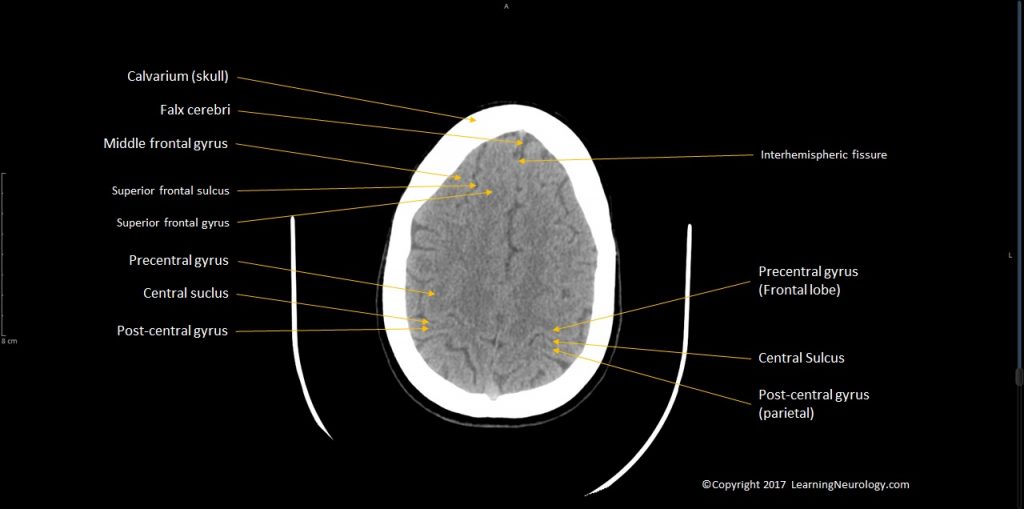
- Skull & scalp
- Ventricles & cisterns & sulci
- Brain matter
- Major vessels, arteries, veins & dural sinuses
- Extended search
- Review areas
Skull & scalp:
- Bruises
- Fractures
- Sclerotic or lytic lesions
- In paediatrics: size & shape
Ventricles & cisterns & sulci:
- Ventricles:
- Lateral ventricles (frontal, occipital & temporal horns), Third ventricle (slit like), fourth ventricle
- Cisterns & fissures:
- Quardrigeminal plate cistern, interpeducular cistern, ambient cistern a.k.a. cistern of the great cerebral vein
- Sulci:
- Appearance: effaced, obscured
- Ventriulo-sulcal proportionality
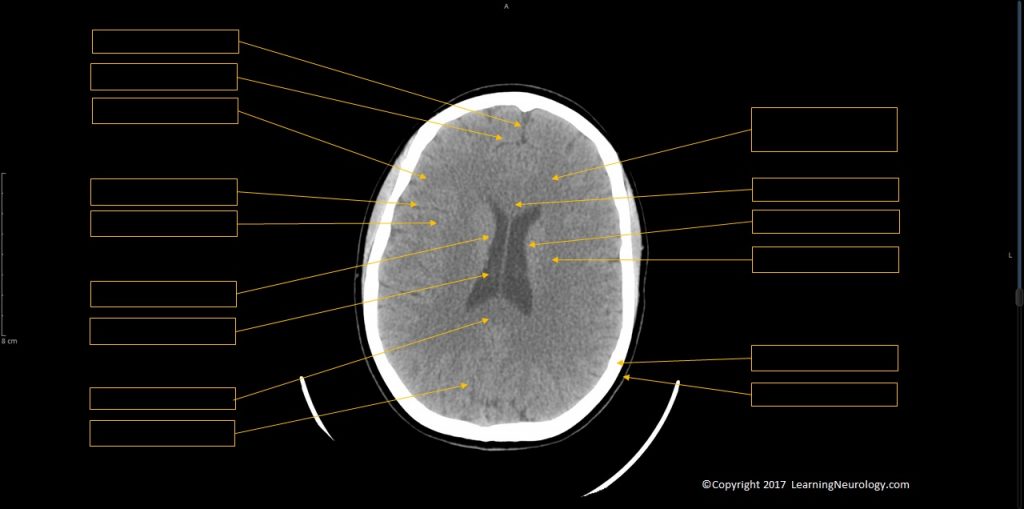
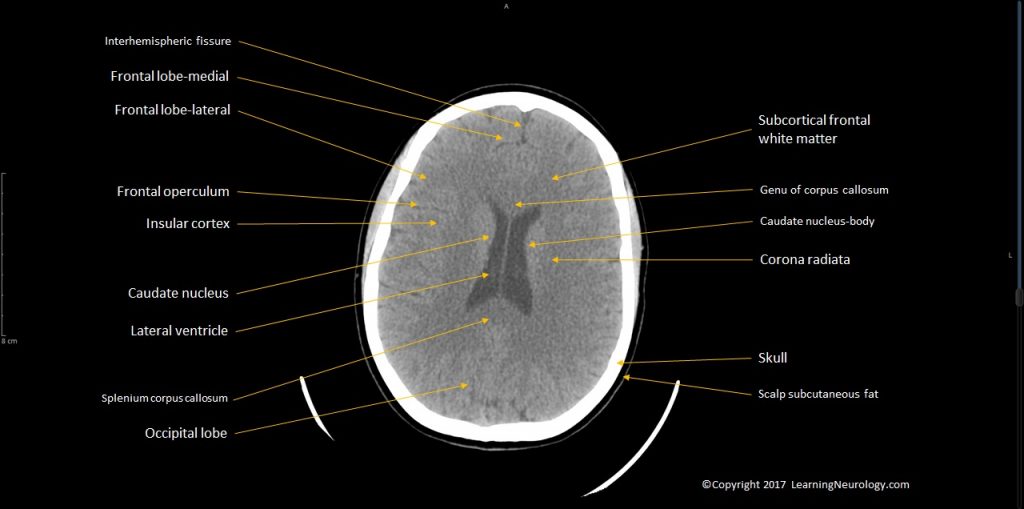
Brain matter:
- Gyral pattern
- Midline shift
- Normal grey-white differentiation
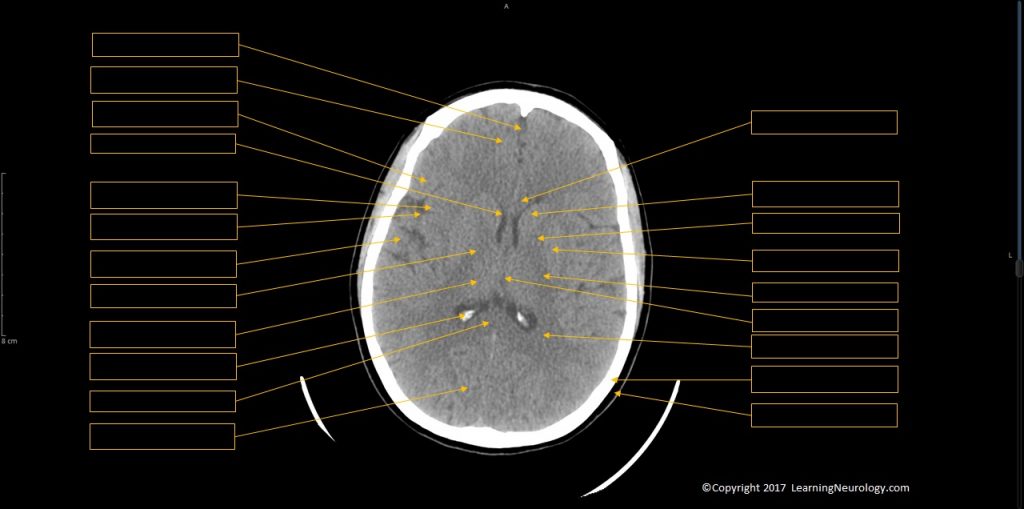
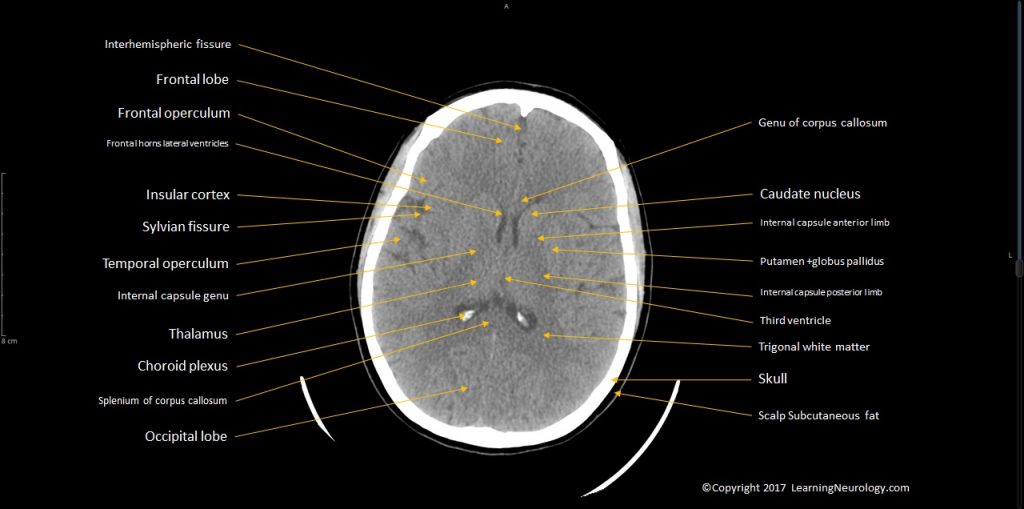
- Identify structures:
- Caudate nucleus
- Internal capsule
- Putamen & globus pallidus
- Thalamus
- Other structures: centrum semiovale, midbrain, pons, medulla, cerebellum
Major vessels, arteries, veins & dural sinuses:
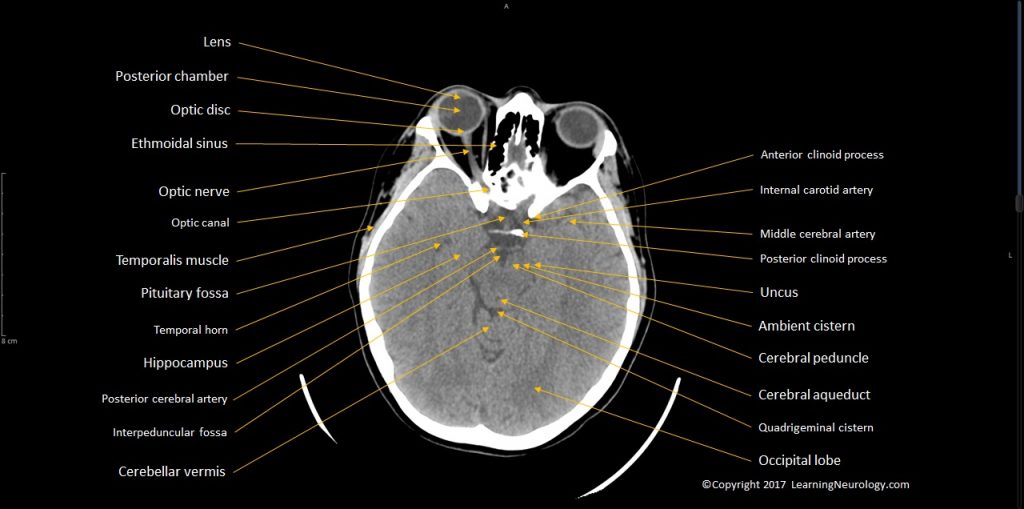
- Internal carotids in the cavernous sinus, MCAs, basilar artery
- Sagittal sinus, torcula, transverse sinus, straight sinus, deep cerebral venous system
Extended search:
- Sella, pituitary & optic chiasm
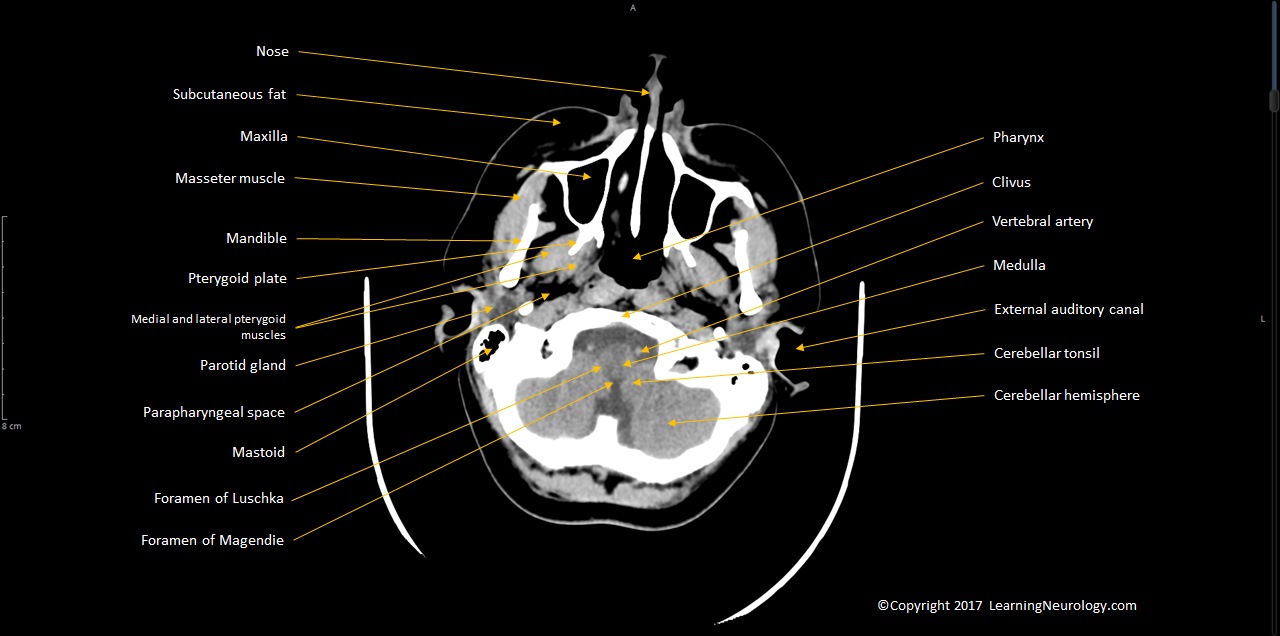
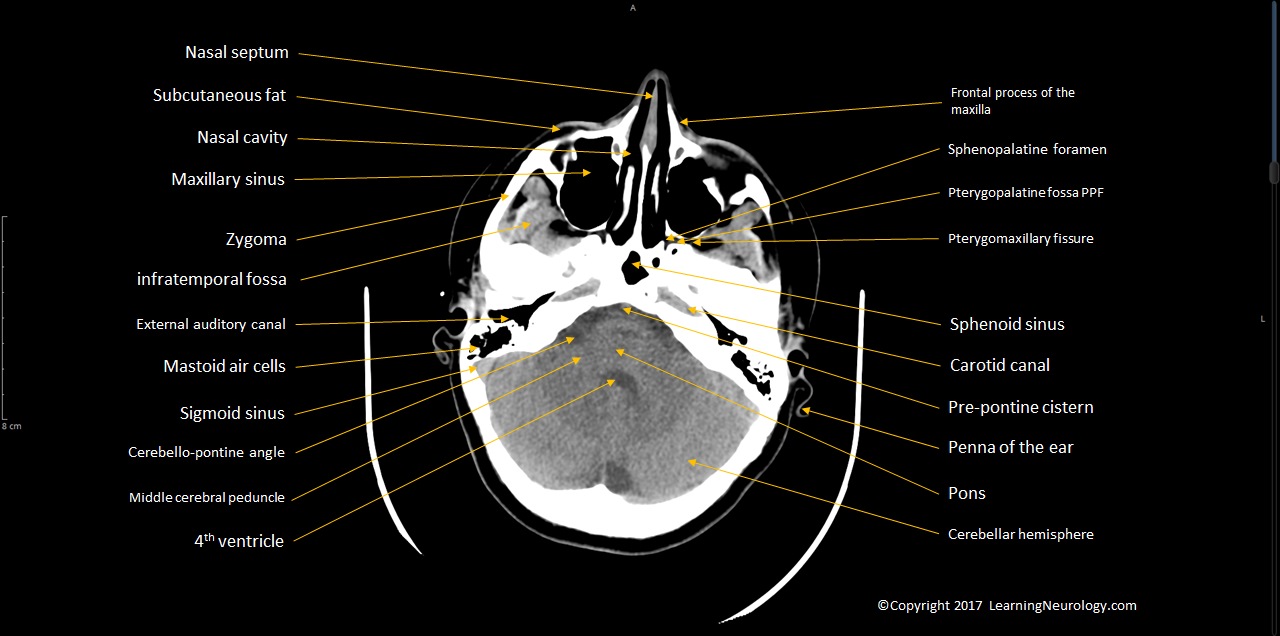
- Paranasal sinuses (ethmoidal, sphenoid, frontal, mastoid), temporal bone/ears
- Orbits
- Nasopharynx, Oropharynx
Review areas:
- Top slices of the hemispheres
- Pituitary & parasellar structures
- Orbits & sinuses
- Craniocervical junction

Editor note:
Interpretation:
Approach to the lesions:
- Single vs. multiple
- Location (which fossa, intraaxial, extraaxial)
- Margin (poorly defined–> infiltration, sharp–> extraaxial)
- Shape (e.g. vascular territory, extradural)
- Homogenous vs. heterogenous
- Associated edema
- Response to contrast
Notes & tips:
- White matter is darker than grey matter.
- Thalami, putamen &globus pallidus are higher density than white matter.
- Cerebral blood flow CBF= MTT mean transit time/Cerebral blood volume CBV
- Look at the top of the brain for sulcal effacement especially in hydrocephalus
In hydrocephalus look at the 3rd ventricle & 4th ventricle and pineal gland (normally calcified) to localise the obstruction.
Causes of hypodensity:
- Edema
- Stroke
- Mass
- Demyelination
- Non-hemorrhagic shearing injuries
- CSF
- Air
- Low protein fluid
Causes of hyperdensity:
- Blood
- Calcification
- High protein fluid
- Metal
- Lymphoma
Hemorrhage vs. tumor:
- High density on noncontrast: blood
- High density only on post contrast: tumour
- Repeat imaging after an interval to assess for hematoma resolution