Abnormal speech and “slurred speech” are some of the commonest problems that neurologists are consulted for. This might occur in the emergency setting, as when trying to determine if the patient is having an acute ischemic stroke to deliver emergent therapy such as thrombolysis or endovascular therapy. Other times, it occurs in the non-emergent setting where you have more time to do a thorough evaluation. It is important to have a plan of how to assess speech and language to determine the underlying cause, and equally it is important to practice this assessment skill.
The first task is to determine whether there a disturbance of speech or is this a mimic such as a disturbance of cognition or disorientation? Remember, as humans we heavily use speech and language to communicate. It is the primary way we determine what other people are thinking. Often patients with delirium present with or are presented as having a speech problem. “Grandma wasn’t making sense, her speech was abnormal so we called 911”. This presentation may represent aphasia, a language disorder, which may indicate an acute ischemic stroke. Alternatively patients with encephalopathy, due to urinary tract infection for example, may present with the same story. Is the patients speech abnormal because of a speech production or language disorder? or is the speech abnormal because the patient has disorientation or cognitive dysfunction? Assessing fluency, comprehension, repetition, naming, articulation, reading and writing will help you determine how to proceed.
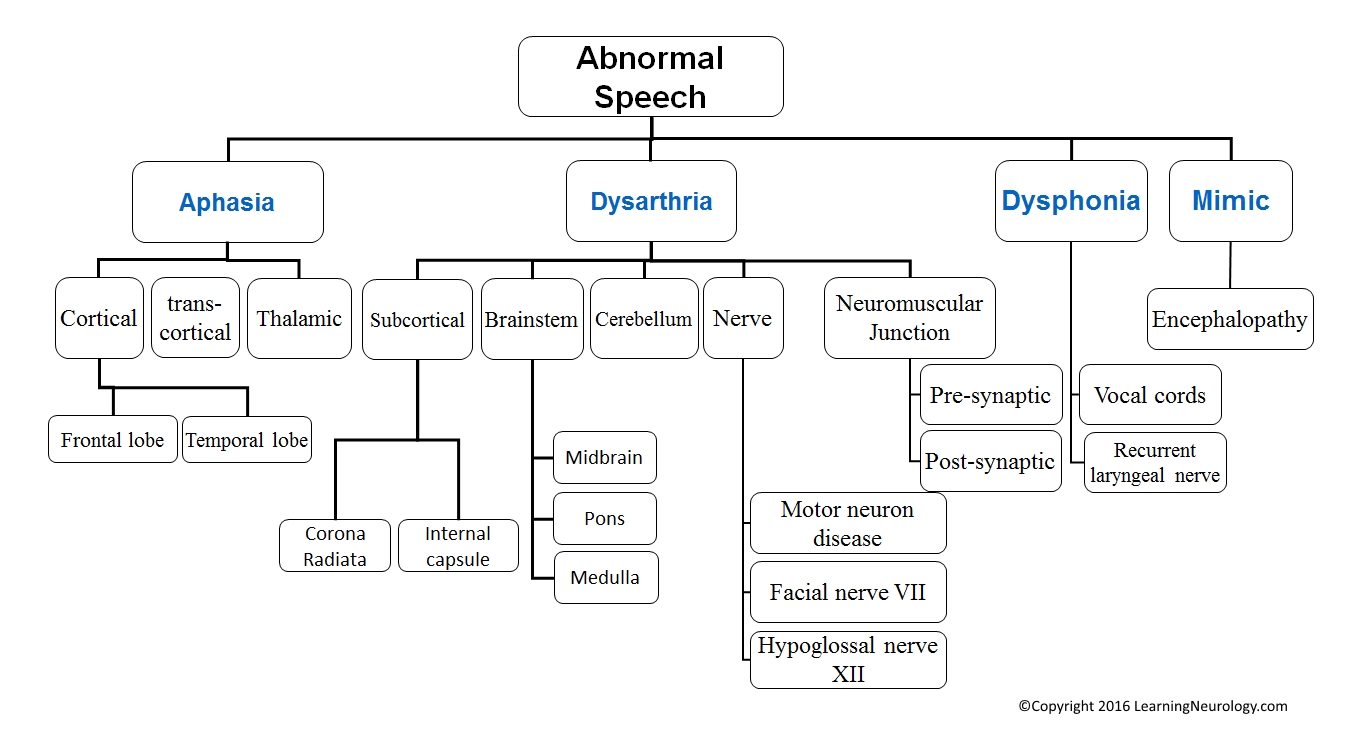
After you have determined that the presentation is indeed a speech problem and not disorientation or a cognitive problem, you should determine whether the speech problem is a language disorder or a disorder of sound/voice production. The aphasias imply that there is a dysfunction of the language centers and networks. Dysarthria and dysphonia indicate that language is intact but speech and voice production are impaired because the motor component of speech production. For example, a patient with bilateral facial weakness due to myasthenia gravis will have normal language centers but impaired speech because the patient can not move the tongue, palate and lips properly to produce speech. On the other hand a patient with left middle cerebral artery occlusion and infarction of the perisylvian frontal lobe (Broca’s area) may not be able to speak because of an expressive aphasia. Again assessing fluency, comprehension, repetition, naming, articulation, reading and writing will help you determine how to proceed (see the Examination of speech section below for an outline of what to assess).
After these two steps, then you can proceed to the usual neurological approach of where is the lesion? what caused the lesion? and what are we going to do about it? For example does the lesion localize to the dominant hemisphere temporal lobe (Wernicke’s area)? Was the onset sudden to suggest an acute ischemic stroke or gradual and progressive to suggest a space occupying lesion such as an astrocytoma. Maybe you identified the problem as dysarthria and then localized it as a lower motor neuron problem of the lower cranial nerves (IX, XII). Here you would think about bulbar palsy and the search for underlying causes for that.
Framework for approaching abnormal speech:
- What is the presentation/problem? Is it a speech and language disorder or is this a mimic like disorientation or cognitive impairment?
- Is this a disorder of language, an aphasia? or is this a speech or voice production problem; dysarthria or dysphonia?
- Where is the lesion?
- What caused the lesion?
- What are we going to do about it?
Terminology & localization:
- Dysphasia ~ Aphasia: a disorder of language, or disorder of generation, understanding & content of speech. Usually patients aphasic in speech are also aphasic in writing
- Receptive dysphasia: inability to comprehend (understand) speech. Wernicke’s area (temporal lobe)
- Expressive dysphasia: inability to express using speech despite adequate comprehension. Broca’s area (frontal lobe)
- Global dysphasia: inability to comprehend or express speech both Wernicke’s & Broca’s areas
- Nominal dysphasia: inability to name objects
- Conductive aphasia: inability to repeat, with normal comprehension & fluency. Arcuate fasciculus &/or supramarginal gyrus
- Dyslexia: inability to read
- Dysgraphia: inability to write
- Dysarthria: difficulty in articulation, or difficulty in coordination of the structures producing speech or pronunciation
- Causes of dysarthria:
- Cerebellar disease
- Pseudobulbar palsy i.e. Upper motor neuron (UMN) lesion
- Bulbar palsy i.e. Lower motor neuron (LMN) lesion
- Facial nerve palsy e.g. Bell’s palsy
- Extrapyramidal disease
- Oral candidiasis
- Stutter
- Dysphonia: impaired voice production, impaired phonation laryngitis or vagal nerve damage
- Other points:
- A patient who can’t speak but can write is mute, there are many causes of this e.g. rigidity, bilateral UMNL, LMNL to the vocal cords, psychiatric illness
- Patients that have dysarthria rather than dysphasia can write well.
- Nominal aphasia doesn’t localise to a specific area, the causes include metabolic disturbances (i.e. encephalopathy) or diffuse structural lesions.
- Broca’s aphasia is often associated with a hemiparesis, and localises to frontal lobe lesions
- Wernicke’s aphasia is often associated with a visual field deficit, and localises to temporal lobe lesions
- If functions other than language are impaired, think of metabolic causes or diffuse lesions.
- If only language is impaired, think of the dominant lobe lesions
- Dysphonia with a normal cough implies laryngeal lesions, dysphonia with a bovine cough implies vocal cord lesions
- Causes of dysarthria:
Examination of speech:
- Free (prepositional) speech:
- “Can you describe the room?”
- “Can you tell me your name & address?”
- Test comprehension:
- Ask to follow an order: (don’t demonstrate)
- ‘close your eyes’, ‘stick out your tongue’, ‘point to the door’
- Yes/no questions
- Ask to follow an order: (don’t demonstrate)
- Repeating a phrase, ask the patient to repeat one of the following phrases:
- “Today was a nice day”
- “West register street”
- “British constitution”
- “Baby hippopotamus”
- “No ifs, ands, or buts”
- Naming an object:
- Pen, Watch, Coin
- If they can’t, ask them if they know what it does or what it’s used for
- Reading
- Writing
- To test the movements of speech:
- PPP, tests the lips
- TTT & LLL, tests the tongue
- KKK, tests the palate
- To test for dysphonia:
- Can you cough please?
- Say “eeeeeeeee”