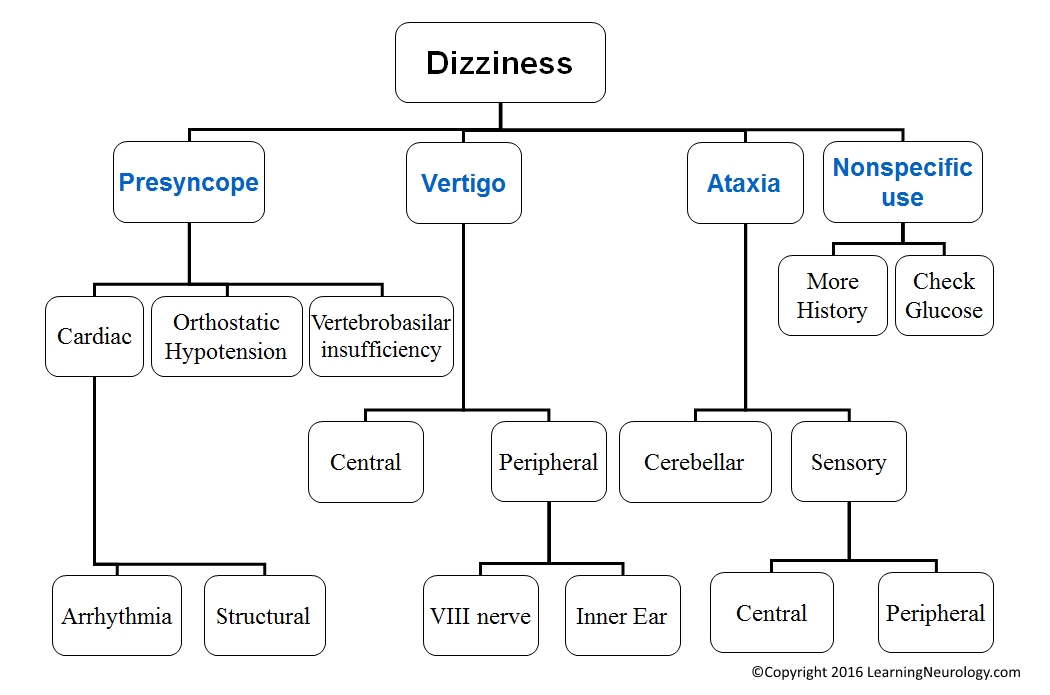
Dizziness should be clarified by history as one of the following:
- Vertigo
- Pre-syncope
- Ataxia
- Non-specific use of the word dizziness
Features on History:
Assess what happened first
- Examples:
- Hearing loss first and then vertigo later on suggests otosclerosis.
- Fluctuating hearing loss associated with vertigo suggests Meniere’s disease.
Features of Central causes:
- Usually less nausea or vomiting. Some other neurological symptoms are usually present.
Features of peripheral causes:
- Peripheral causes have very different features depending on the cause, so it is best to read up on the individual causes (see below). Having said that, otological causes of vertigo have no other neurological symptoms apart from hearing loss or tinnitus. No diplogia, dysphagia, dysarthria, weakness or numbness. See below for the physical exam features.
Assess Temporal features:
- Onset is always sudden i.e. one either has vertigo or not. It doesn’t build up. Lasting seconds, minutes or hours. Intermittent vs. persistent.
- Examples:
- Episodes lasting seconds suggests Benign paroxysmal positional vertigo.
- Episodic vertigo lasting minutes to hours suggests Meniere’s disease.
- A single episode lasting hours to days suggests acute vestibular neuritis (acute peripheral vestibulopathy) or central causes
- Preceeding events:
- Head trauma: Postraumatic vertigo (Cupulolithiasis)
- Ear infection/surgery/trauma: Perilymph fistula
- Drugs: aminoglycosides
- Subsequent events:
- Headache: basilar artery migraine
- Associated features:
- Diplopia, slurred speech, perioral numbness, dimming of vision, drop attacks: vertebrobasilar TIA.
- Vomiting at onset: vestibular neuronitis.
- Severe ear or facial pain: Ramsay-Hunt Syndrome VZV
- Important: Establish character of initial “dizzy” episode as with recrurrent episodes vertigo becomes lightheadedness
- Important: Vertigo of any cause is worsened by head movement. However, establish whether the symptom of vertigo completely goes away if the patient stays perfectly still. In BPPV vertigo should disappear after staying still. In vestibular neuritis the symptom may continue even without head movement.
Examination of The patient with vertigo:
- Otoscopy
- Tuning fork tests:
- Weber’s & Rinne’s
- Neurological examination (full screening exam but pay attention to the following):
- Cranial nerves:
- II, III
- V
- VII, VIII
- IX, X, XII
- Cerebellar testing
- Nystagmus
- Romberg’s test: propreception ‘joint position’
- Unterberger’s stepping test: >30 degree rotation to the side of the lesion
- Tandem gait test ‘heel shin test’
- Cranial nerves:
- Important test: Dix Hallpike test a.k.a. Nylen Barany test
- Hyperventilation test: 1 minute, (psychogenic causes)
“H.I.N.T.S.” Battery (Head Impulse, Nystagmus, Test of Skew), stroke will usually have one or more of the following:
- Normal horizontal head impulse test (in complete or severe vestibular neuritis this is unilaterally abnormal)
- Fast-phase alternating nystagmus in stroke: the fast phase of nystagmus alternates by right and left lateral gaze (in vestibular neuritis it is direction-fixed nystagmus i.e. the fase phase is always in one direction)
- Skew deviation occurs in stroke (this is assessed by the alternating cover test, look for refixation)
- Reference:
- Saber Tehrani AS et al. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology. 2014 Jul 8;83(2):169-73. doi: 10.1212/WNL.0000000000000573.
Interpretation:
- Patients with peripheral causes of vertigo should have a normal neurological exam apart from some hearing loss and nystagmus. There should be normal eye movements apart from nystagmus i.e. no skew deviation or refixation on the alternating-cover-test
- Peripheral vestibulopathy:
- Nystagmus with the fast-phase away from the lesion.
Causes of vertigo:
Peripheral vestibular causes, ~90%:
- Middle ear:
- A complication of: (eroding thesemicircular canal)
- Chronic otitis media
- Severe acute otitis media
- Perilymph fistula a.k.a. ?Labrynthine fistula
- Otosclerosis, late
- Inner ear:
- Benign paroxysmal positional vertigo BPPV
- Meniere’s disease
- Trauma (Labyrinth damage or VIII nerve damage):
- Temporal bone fracture
- Middle ear surgery
- Vestibulocochlear nerve:
- Acute peripheral vestibulopathy a.k.a Vestibular neuritis a.k.a. vestibular neuronitis
- Ramsay Hunt syndrome, VZV as an additional symptom
- Cerebellopontine angle tumour e.g. Vestibular schwannoma a.k.a. acoustic neuroma. A late feature
- Paget’s disease of the skull
- Recurrent vestibulopathy Dx by exclusion
- Drugs/toxins:
- Alcohol
- Aminoglycosides, salicylates, quinine/quinidine, cisplatin
Central vestibular causes, ~10%:
- Migraine with aura (e.g. basilar type migraine)
- Multiple sclerosis
- Cerebrovascular: posterior circulation TIA, ischemic stroke
- Brain Tumor
Features of the commonest causes of vertigo:
BPPV a.k.a. Benign paroxysmal positional nystagmus BPPN:
- History: <1 minutes, episodic vertigo, +/-nausea, associated with certain head positions.
- Dix-Hallpike test or Nylen-Barany maneuver:
- Starting position: sitting 90 degrees
- End position:
- Flat supine
- Head 45 degrees below bed
- Head rotated 45 degrees to one side
- Test eye movements
- Repeat test with head to the other side
- Results: Nystagmus +/-vertigo
- Central gaze: Nystagmus is vertigal upwards with rotation towards the lower ear.
- Gaze to the lower ear: Fast-phase of nystagmus is towards lower ear.
- Gaze to the upper ear: Fast-phase of nystagmus is upwards.
Vestibular neuritits:
Synonyms:
- Acute peripheral vestibulopathy a.k.a. Vestibular neuritis, labrynthitis and “viral neurolabrynthitis” a.k.a. recurrent peripheral vestibulopathy
Clinical:
- Single or recurrent, true vertigo, hours or days, initially associated with vomiting. May be worsened by head movement. Slow recovery, days or longer.
- Vestibular neuronitis= if without hearing loss
- Labrynthitis= if with hearing loss
Meniere’s disease:
- History: 40-60 y.o. with episodic vertigo lasting minutes to hours, fluctuating sensineural hearing loss, tinnitus & aural fullness, may have an aura (fullness, tinnitus)
- Physical exam during an attack: nystagmus, positive Romberg’s test, deviation on walking with eyes closed. Dix-Hallpike test may be positive indicated co-existing benign positional vertgo.
- Audiology: decreased bone conductance in low frequencie, later on all frequencies are affected
- Consider electrocochleography EcoG
Perilymph fistula PLF:
- Clinical: sensineural hearing loss, tinnitus, paroxysmal vertigo, disequlibrium, aural fullness. Occurs after excursion e.g. childbearing or heavy lifting
- Fistula test: Clinical or electronystagmogram Fistula test + impedance bridge
- Consider Exploratory tympanotomy
- Beta 2 transferrin in the fluid at the oval window by western blott
- Audiology: for sensineural hearing loss
- MRI, T1 Gadolinium enhanced: to exclude cerebellopontine angle lesions
- If child, CT temporal bone: for anomalies of the ear
- ECoG electrocochleogram: for raises SP/AP ratio
Vestibular schwannoma:
Clinical:
- Early: tinnitus, hearing loss (sensorineural), vertigo
- Late: cerebellar signs, hemiplegia, bulbar signs
MRI, with & without contrast:
- Cerebellopontine angle mass
- Extends into the internal auditory canal IAC
- Enhances with contrast
Stroke causing vertigo:
Clinical:
- Usually is accompanied by other neurological findings
Cerebellar & brainstem - The nystagmus doesn’t extinguish, may be in any direction but stays in the same direction
“H.I.N.T.S.” Battery (Head Impulse, Nystagmus, Test of Skew), stroke will have one or more of the following:
- Normal horizontal head impulse test (in vestibular neuronitis this is unilaterally abnormal)
- Fast-phase alternating: the fast phase of nystagmus alternates by right and left lateral gaze (in vestibular neuritis it is direction-fixed nystagmus i.e. the fase phase is always in one direction)
- Skew deviation occurs in stroke (this is assessed by the alternating cover test, look for refixation)
- reference:
- Saber Tehrani AS et al. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology. 2014 Jul 8;83(2):169-73. doi: 10.1212/WNL.0000000000000573.
Mechanism/vessels:
- PICA: posterior inferior cerebellar artery
- Artery to artery (dissection or atherosclerosis)
- Or cardioembolic
- Small vessel perforators from the basilar artery: i.e. lacunar stroke
- Vertebral artery occlusion
Causes of brain hypoperfusion ‘syncope’:
- Neurally mediated syncope: (old names & related terms; Reflex mediated, Vascular tone & related):
- ‘simple faint’ a.k.a. Vasovagal reflex a.k.a. vasodepressor-bradycardic a.k.a. neurocardiogenic, central emotional stimulus
- Reflex/Situational syncope:
- Valsalva & Valsalva like: Cough, defaecation
- Micturation
- Deglutition
- Hyperventilation syncope
- Carotid sinus hypersensitivity
- Hemodynamic stress/orthostatic intolerance
- Glossopharyngeal neuralgia or trigeminal neuralgia
Orthostatic hypotension a.k.a. postural hypotension (see causes)
Cardiac syncope:
- Arrhythmias
- Inflow obstruction:
- Left atrial myxoma or thrombus, severe mitral stenosis
- Constrictive pericarditis or cardiac temponade, Restrictive cardiomyopathies
- Tension pneumothorax
- Outflow obstruction:
- Aortic stenosis
- Hypertrophic cardiomyopathy
- Acute pulmonary embolus
- Atrial myxoma
- Dissection of the aorta
Cerebrovascular syncope:
- Vertbrobasilar ischemia (ischemic stroke or transient ischemic attack)
- Subclavian steal syndrome
- Migraine
- Takayasu’s disease
Causes of ataxia:
Cerebellar ataxia:
- See causes of cerebellar ataxia
Sensory ataxia:
- See causes of sensory ataxia
Vestibular ataxia:
- See ‘vertigo’ peripheral vestibular causes
- See ‘vertigo’ central vestibular causes
Causes of cerebellar ataxia:
Acute:
- Vertebrobasilar ischemia and infarction
- Cerebellar hemorrhage
- Drugs/toxins:
- Ethanol, phencyclidine
- Phenytoin, Benzodiazepines,
- B1 deficiency a.k.a. Wernicke’s encephalopathy (ataxia, confusion, ophthalmoplegia)
- Viral encephalitis:
- St. Louis encephalitis, AIDS dementia complex, VZV, mumps, poliomyelitis,
- EBV, lymphocytic choriomeningitis
- Bacterial: abscess,
- Acute cerebellar ataxia of childhood
- Acute disseminated encephalomyelitis (ADEM)
- Miller-Fisher variant of Guillain-Barre syndrome (ataxia, ophthalmoplegia, areflexia)
Chronic:
- Multiple sclerosis
- Alcoholic cerebellar degeneration
- Phenytoin-induced cerebellar degeneration
- Hypothyroidism
- Brain Tumor
- Paraneoplastic cerebellar degeneration
- Autosomal dominant spinocerebellar ataxia:
- Friedreich’s ataxia
- Spinocerebellar ataxia SCA type 1-17
- Ataxia telangiectasia
- Wilson’s disease
Causes of sensory ataxia:
Peripheral sensory neuropathy:
- Diabetes
- Hypothyroidism
- Diphteria
- Immune:
- GALOP syndrome, anti-MAG syndrome, Miller Fisher syndrome, anti-GD1b antibody syndrome
- Paraneoplastic anti-Hu antibody
- Drugs:
- Isoiazid, Pyridoxine, Cisplatin, Paclitaxel
- Hereditary:
- Autosoma dominant sensory ataxic neuropathy
- HMSN-type III (Dejerine-Sottas disease)
- Refsum’s disease
- Those that may also affect the posterior columns, see below
Sensory nerve root lesions
Myelopathy: (Posterior columns)
- Multiple sclerosis
- Acute transverse myelitis
- Spinal Cord compression e.g. Tumour
- Spinal Vascular malformation
- AIDS vacuolar myelopathy
- Those that also may affect the peripheral nerves:
- Friedreich’s ataxia
- Neurosyphilis (tabes dorsalis)
- Nitrous oxide
- Vitamin B12 deficiency a.k.a. subacute combined degeneration of the spinal cord
- Vitamin E deficiency
Medial lemniscus lesions, rare
Thalamic lesions (hemi-ataxia or gait ataxia), rare
Parietal lobe lesions (hemi-ataxia), rare