This section explains an approach to assessing the patient with sensory deficits or complaints that leads to a more efficient and comfortable tailored investigation and treatment plan. The list of causes of sensory deficits is very long and encompasses the whole somatic nervous system: brain, spinal cord and peripheral nervous system. Imagine ordering MRI of the whole neuroaxis, NCS/EMG and all the peripheral nervous system lab test for every patient with numbness or sensory disturbance! What if after all that the diagnosis is still illusive? That is an inefficient and uncomfortable way to assess the patient. Luckily we do not have to practice medicine that way.
Similar to focal motor deficits the approach to sensory deficit also involves the four general steps of approaching neurological symptoms. The first step is to determine whether patient’s complaints represents a focal sensory deficit or another neurological presentation or non-neurological presentation. For example the patient may use the word numbness when they mean that there are weak and that they’re trying to describe a loss of motor power. Clarify what the patient means and whether there is a sensory deficit. The next step involves answering the question “where is the lesion within the sensory part of the nervous system?”. Remember that there are two main sensory systems in the central nervous system; the spinothalamic tract and the dorsal column pathway. Also remember that sensory deficits may occur from central nervous system disease as well as peripheral nervous system disease. Step number three involves answering the question “what caused the lesion? “. This question reminds us to look for the etiology that may best fit with the patient’s temporal and associated features at the lesion location. This gives us the differential diagnosis. The final step in approaching patients with sensory deficits involves devising an investigation and treatment plan based on a differential diagnosis.
The usual sensory problems are numbness, paraesthesia and problems due to proprioception loss. Theses are the things to detect on the history. A useful simple question is “does it feel normal or abnormal when things touch your skin?”. Then clarify whether the sensation is absent, partially lost or associated with other features. For example some patients will not a discomfort that accompanies the numbness e.g. burning sensation to touch. This is called dysesthesia. However, loss of sensation is often painless. Sensory symptoms can range from subtle to prominent. There are patients who will not notice the sensory deficits and may have scratches, ulcers or burns in areas of sensory loss that they are unaware of. Your physical examination may be the first clue that there is a sensory deficit. In other patients they may complain that they can not feel on one area or that they have “positive” symptoms such as paraesthesias (tingling). Patients with loss of proprioception and vibration sense may complain about falling or being clumsy as the sensory input from these modalities is necessary to plan movement. This is particularly relevant with the other compensatory mechanisms such as visual input are not available. For example a patient with proprioception loss due to vitamin B12 deficiency induced dorsal column disease may fall at night in when in a dark room. This occurs more often at night because during the day the patient compensates by using visual input to “tell his brain” where the limbs are positioned in space.
An important note on pain. Pain is a sensory modality. It is more difficult to use pain for localization. This may be because pain doesn’t always follow strict dermatomes in radiculopathy and because there is modulation of pain in the spinal cord and in the brain that makes it difficult to test. Distribution of pin-prick loss and presence or absence of vibration and proprioception as much more useful in localization.
The main modalities that are tested on physical exam are pin-prick and sometimes temperature for the spinothalamic tract, and proprioception and vibration for the dorsal column system. It takes time and practice to learn how to incorporate this in your practice. The sensory exam can be efficient and useful. There are many ways to use it, but it can be tailored to the individual patient. For patients we are not suspecting a sensory problem or where it is of less diagnostic important, a simple screen with light touch is usually sufficient; for example, in large vessel stroke syndromes. However, in patients where it is of localizing value a more detailed yet efficient exam is called for; for example using pin-prick for each dermatome and then testing distally for vibration and proprioception when a radiculopathy or polyneuropathy or small fibre neuropathy is in the differential diagnosis. It is also important to mention that a sensory level using pin-prick and testing for proprioception and vibration is mandatory when spinal cord disease is suspected. Testing sensation requires some degree of consciousness and blinding. Learn from your supervising neurologists or the neurological exam text books an efficient way to do this while maintaining objectivity.
Where is the lesion?
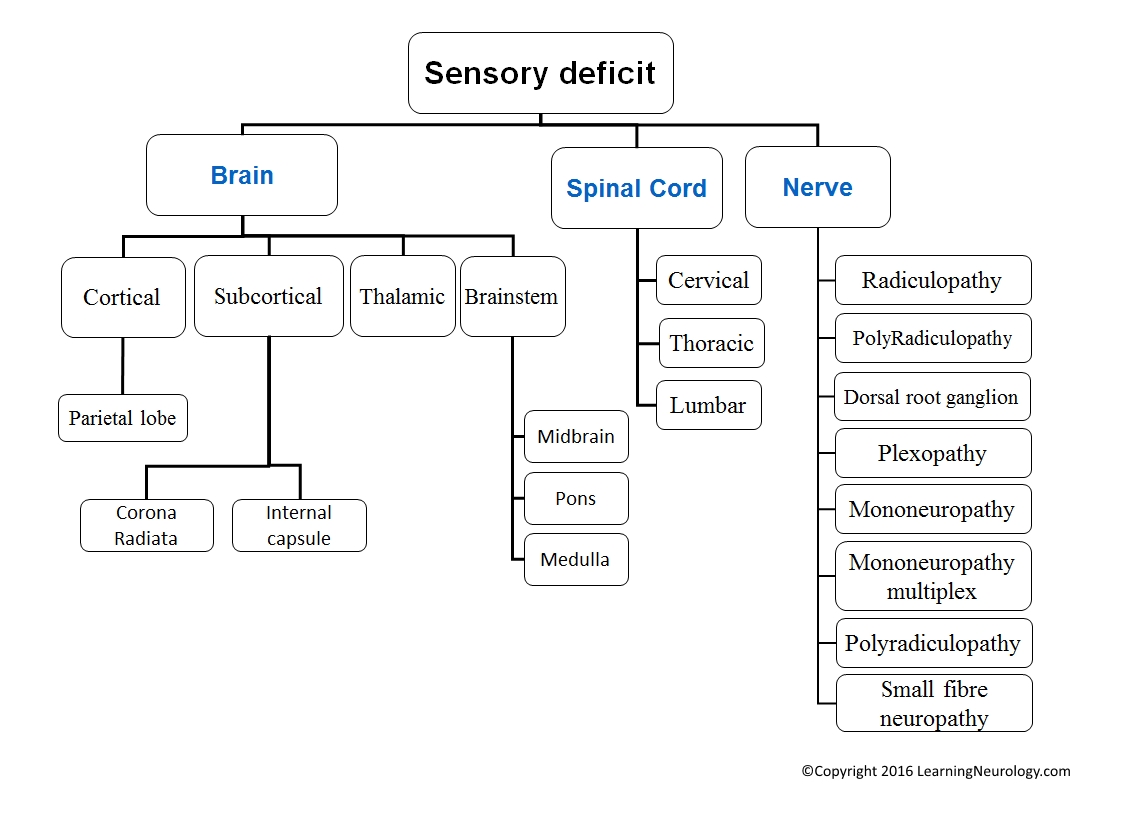
As a brief note on localization, it is useful to take time to think of the sensory pathways and locations of possible lesion dysfunction backwards from the parietal lobe to the peripheral nerves. Sensory deficits can occur due to disease of the parietal lobe, the subcortical white matter, the thalamus, the ascending pathways in the pons and brainstem, spinal cord disease (anteriorly and laterally for spinothalamic tract, and posteriorly for dorsal column disease), the sensory nerve roots, the dorsal root ganglia and the peripheral nerve (this may be separated into large fibre and small fibre). As you work your way down these locations think about what pattern of sensory problem they will produce? whether or not there will be cortical symptoms or signs? whether there will be cranial nerve symptoms or signs? what the distribution will be which limb or limbs, one limb, hemisensory loss, bilateral lower limbs or all limbs?
For spinal cord lesions think about bowel and bladder and erectile dysfunction and presence of a sensory level? When you find a sensory level try to determine whether sensation is abnormal below the level. If it is then the lesion likely occupies involves the ascending spinothalamic tract laterally. Most myelopathies like multiple sclerosis, compressive myelopathies and transverse myelitis will fit into this. If sensation is intact below the sensory level and above the sensory level, then the patient has a “suspended sensory level”. This indicates a lesion of the spinothalamic tract as it crosses within the spinal cord. Typically this is caused by syringomyelia. Also try to determine whether the dysfunction is in the anterior spinothalamic system, or the posterior dorsal column system, or both. This will help you localize within the axial plane of the spinal cord. The causes are different depending on location. Lastly for spinal cord lesions as with motor deficits try to determine whether the lesion is in the cervical, thoracic or lumbar spinal cord as different diseases affect different parts.
For the peripheral disorders think about the general distribution of the peripheral nervous system regarding radiculopathy, plexopathy, mononeuropathy, polyradiculopathy, polyneuropathy and others? Also for the peripheral nervous system localization of sensory disturbances think about large fiber neuropathies (involves reflexes, and possibly vibration and proprioception) vs. small fibre neuropathies (spares reflexes). The lists with descriptors below and the section on neuromuscular disease patterns may be useful as you work through this.
What caused the lesion?
There are some very common conditions that cause sensory deficits. A few important conditions are sensory loss or paraesthesia with multiple sclerosis in the form of myelopathy or difficult to localize single lime numbness, hemisensory loss with thalamic stroke, proprioception loss unilaterally in parietal stroke, distal symmetric sensory loss in polyneuropathy especially with diabetic polyneuropathy and mononeuropathy as with carpal tunnel syndrome. There are less common conditions that are worth mentioning such as sensory ganglionopathy (idiopathic or paraneoplastic destruction of the dorsal root ganglion) and small fibre neuropathy because they illustrate the organization and localization of sensory deficits. With sensory ganglionopathy the patient will have a profound loss of sensation, in particular proprioception loss, and this can lead to a sensory ataxia. Thankfully, it is a rare condition. Small fibre neuropathy is worth mentioning because it highlights that there is a localization value to realizing that the peripheral nerves have large myelinated fibres and small unmyelinated fibres. In conditions where the small fibres are damaged without damage to large fibres, the patient will have sensory symptoms or findings but will have intact reflexes in spite of having peripheral nerve damage. This is because reflexes use the large myelinated fibres as the anatomical substrate. Amyloidosis is a cause of small fibre neuropathy. See this list below for some clarification.
Features by localizations for sensory symptoms:
Cerebral cortex:
- May be associated with dysfunction of higher centers e.g. Broca’s aphasia etc.
- May conform to the territory supplied by one of the cerebral arteries:
- Contralateral Legs: anterior cerebral artery
- Contralateral Face and arm: middle cerebral artery
- Vision: posterior cerebral artery
- Hemiparesis: middle cerebral artery
- If parasagittal, it affects both legs and then maybe both arms
- Subcortical lesions can produce similar symptoms to the cortical ones.
Centrum semiovale and Coronal radiata:
- Usually face or arm or leg or combination without equal involvement of all three.
- This can be difficult to localize, and in the past has led a lot of patients to being dismissed incorrectly as psychogenic.
- Subtle lesions in this area are common with multiple sclerosis. This can range from asymptomatic to “non-specific” numbness pattern in a limb that doesn’ fit with radiculopathy or mononeuropathy or plexopathy
Internal capsule:
- Usually a severe “dense” hemiparesis with or without sensory symptoms, because the fibres are packed closed to one another.
Thalamus:
- Sensory:
- Loss of sensation of one half of the body, pain in one half of the body
- Thalamic pain a.k.a. thalamic syndrome: pain on touching the skin
- Motor: hemiparesis, less common than sensory dysfunction
- Cognitive dysfunction because of reciprocal connections with the cortex:
- Frontal network syndrome may occur; i.e. symptoms/signs of frontal lobe disease
- Aphasia may occur with left-sided lesions.
- Agnosia may occur with right-sided lesions.
- Decreased level of consciousness due to interruption of the reticular activating system
Brainstem:
- Cranial nerve involvement
- The D’s of brainstem lesions:
- Diplopia ‘Double vision’, dysphagia, dysarthria, ‘dizziness’ Vertigo and ataxia
- Crossed deficits may occur: e.g. with a left-sided lesions: a facial palsy on the left side and hemiparesis of the right side
- The D’s of brainstem lesions:
- Bilateral signs may occur e.g. quatraparesis
- Later on or in larger lesions, respiratory function may be impaired
- Lhermitte’s sign might occur in cervical myelpathy
- If above C5: quadraparesis more commonly than hemiparesis that spares the cranial nerves
- If below T1: the arm is completely spared but the legs are affected
- A sensory level is very helpful
- Lesions are usually bilateral:
- Associated with bladder or sexual dysfunction
- If unilateral:
- Ipsilateral motor deficit, vibration and proprioception impairment
- Contralateral loss of pain and temperature
- a.k.a. Brown-Sequard syndrome
- A focal lesion may cause an associated lower motor neuron (LMN) lesion at the level, especially if the process also affects the nerve root, we call this a myeloradiculopathy (this is rare though)
- T1-T9 lesions interrupting the sympathetic outflow, Neurogenic shock may occur: this is a form of distributive shock occurring with bradycardia and loss of vascular tone ‘hypotension’. T1-T4 innervate the heart, T5-T9 innervate the vessels
Peripheral nerve:
- Radiculopathy:
- LMNL due to nerve root disease
- In other words, the deficit conforms to the segmental innervation of the affected motor roots
- Sensory modalities e.g. Pain may be a feature, for example sciatica with weakness
- Plexopathy (brachial or lumbosacral):
- LMN lesion due to damage of a plexus (brachial or lumbar)
- The deficit that does not conform to mononeuropathies or polyneuropathy
- Upper arm and shoulder involvement in upper branchial plexus lesions, forearm and hand involvement in lower brachial plexus lesions.
- Mononeuropathy:
- LMN lesion due to single nerve disease
- The deficit conforms to the distribution of a single nerve, e.g. ulnar nerve palsy or radial nerve palsy, median nerve palsy
- Sometimes the nerve is palpable
- Tinel’s phenomenon may occur: tapping the nerve causes a tingling sensation
- Mononeuritis multiplex:
- LMN lesions that begin like a mononeuropathy, but other nerves then become involved
- Therefore it starts asymmetrically i.e. in one arm then progresses to involve other nerves in other limbs
- If seen at the late stage, the disease is diffuse and symmetrical. Therefore the history and progression is important in this case
- Sometimes the nerve is palpable
- Tinel’s phenomenon may occur: tapping the nerve causes a tingling sensation
- Polyneuropathy:
- Develops symmetrically and distally leading to a glove and stocking distribution
- It doesn’t fit into a nerve root (segmental) or multiple peripheral nerve distribution
- Motor, sensory or both
- If sensory: small fibres, large fibres or both
- Small fibres: decreased pinprick and temperature sensation (painful and burning), autonomic dysfunction, but relative sparring of power and reflexes
- Large fibres: areflexia, sensory ataxia
- Small fibre sensory neuropathy
Patterns for localising motor or sensory deficits:
Lateralised symptoms (e.g. hemiparesis):
- Hemispheric lesions
- Thalamus
- Brain stem
- Less commonly, spinal cord
- Associated with cortical signs (aphasia, apraxia, visual field defect):
- Think of hemispheric lesions
- Associated cranial nerve dysfunction (vertigo, diplopia, dysarthria, ataxia):
- Think of brainstem lesions
Cranial nerve abnormalities:
- Ocular: cranial neuropathy III, IV, VI or midbrain or pons
- Facial: cranial neuropathy VII (motor), V (sensory), or pons
- Bulbar: cranial neuropathy IX, XII, or medulla
One limb or Part of a limb is affected:
- Cortical lesion
- Nerve root (radiculopathy)
- Mononeuropathy
- Early mononeuritis multiplex
All limbs are affected:
- Cervical spinal cord lesions
- Brainstem lesions (accompanied by cranial nerve findings)
- Peripheral neuropathy:
- Polyneuropathy
- Polyradiculopathy
- Mononeuroritis multiplex
Only lower limbs affected:
- Thoracic spinal cord lesions
- Lumbar spinal cord lesions
- Peripheral neuropathy:
- Polyneuropathy
- Polyradiculopathy
- Mononeuroritis multiplex
Causes of sensory deficits:
Cerebral cortex:
- Ischemic stroke (parietal)
- Hemorrhagic stroke (lobar hemorrhages), due to cerebral amyloid angiopathy, cavernous malformations, cerebral arteriovenous malformations
Centrum semiovale and Coronal radiata:
- Multiple sclerosis
- Other white matter diseases less commonly
- Brain tumors
Internal capsule:
- Ischemic stroke due to small vessel disease or larger artery atherosclerosis occluding perforator vessels
Thalamus:
- Ischemic stroke due to small vessel disease, cardioembolism or large artery atherosclerosis
- Thalamic intracerebral hemorrhage
- Cerebral Venous sinus thrombosis (although usually presents with headache and other features)
- Brain tumors e.g. low grade astrocytoma
Brainstem:
- Ischemic stroke
- Listeria rhombencephalitis
- Small vessel vasculitis
- Multiple sclerosis
- Multiple sclerosis
- Combined subacute degeneration of the spinal cord (B12 deficiency)
- Cervical spondylosis (osteoartheritis), cervical spondylothisthesis and compressive myelopathy
- Radiation myelopathy
- Syringomyelia (suspended sensory level)
- Most causes of myelopathy will cause some sensory dysfunction
Peripheral nerve:
- Radiculopathy:
- Usually compressive: herniated disc disease, degenerative disc disease, cervical or lumbar spondylosis (osteoartheritis), spondylolisthesis
- Polyradiculopathy:
- Chronic inflammatory demyelinating polyradiculopathy (CIDP)
- Plexopathy (brachial or lumbosacral):
- Tumor or radiation induced
- Idiopathic plexopathy
- Diabetic amyotrophy (motor symptoms are much more prominant)
- Mononeuropathy:
- Carpal tunnel syndrome (median nerve)
- Ulnar neuropathy
- Othe compressive neuropathies
- Mononeuritis multiplex pattern:
- Multiple causes usually with motor deficits as well. Also Lewis Sumner syndrome, Sjogren’s syndrome
- Dorsal root ganglion:
- Paraneoplastic sensory ganglionopathy
- Idiopathic sensory ganglionopathy
- Sjogren’s syndrome
- Polyneuropathy:
- Sjogren’s syndrome
- Coeliac disease neuropathy (gluten neuropathy)
- Diabetic neuropathy (sensorimotor)
- Amyloidosis (small fibre neuropathy)
- See long list in other sections for example nerve disease
- Small fibre sensory neuropathy
- Amyloidosis (small fibre neuropathy)